Endnotes:
1. National Center for Health Statistics, "Fast Stats", Deaths/Mortality Preliminary 2001 data
2. Dr Herbert Ley, in response to a question from Senator Edward Long about the FDA during US Senate hearings in 1965
3. Eisenberg, David M., MD, "Credentialing complementary and alternative medical providers", Annals of Internal Medicine 137(12):968 (December 17, 2002)
4. American Diabetes Association and the American Dietetic Association, The Official Pocket Guide to Diabetic Exchanges (
), McGraw-Hill/Contemporary Distributed Products, newly updated March 1, 1998
5. American Heart Association, "How Do I Follow a Healthy Diet?", American Heart Association
National Center (7272 Greenville Avenue, Dallas, Texas 75231-4596, USA), https://www.americanheart.org
6. Brown., J.A.C., Pears Medical Encyclopedia Illustrated, 1971, p. 250
7. Joslyn, E.P., Dublin, L.I., Marks, H.H., "Studies on Diabetes Mellitus", American Journal of
Medical Sciences 186:753-773 (1933)
8. "Diabetes Mellitus", Encyclopedia Americana, Library Edition, vol. 9, 1966, pp. 54-56
9. American Heart Association, "Stroke (Brain Attack)", August 28, 1998, https://www.amhrt.org;
American Heart Association, "Cardiovascular Disease Statistics", August 28, 1998,
https://www.amhrt.org/;
"Statistics related to overweight and obesity", https://niddk.nih.gov/; https://www.winltdusa.com/
10. "Diabetes Mellitus", Encyclopedia Americana, ibid., pp. 54-55
11. The Veterans Administration Coronary Artery Bypass Co-operative Study Group, "Eleven-year survival in the Veterans Administration randomized trial of coronary bypass surgery for stable angina", New Eng. J. Med. 311:1333-1339 (1984); Coronary Artery Surgery Study (CASS), "A randomized trial of coronary artery bypass surgery: quality of life in patients randomly assigned to treatment groups", Circulation 68(5):951-960 (1983)
12. Trager, J., The Food Chronology, Henry Holt & Company, New York, 1995 (items listed by date)
13. "Margarine", Encyclopedia Americana, Library Edition, vol. 9, 1966, pp. 279-280
14. Fallon, S., Connolly, P., Enig, M.C., Nourishing Traditions, Promotion Publishing, 1995;
Enig, M.C., "Coconut: In Support of Good Health in the 21st Century", https://www.livecoconutoil.com/maryenig.htm
15. Houssay, Bernardo, A., MD, et al., Human Physiology, McGraw-Hill Book
Company, 1955, pp. 400-421
16. Gustavson, J., et al., "Insulin-stimulated glucose uptake involves the transition of glucose transporters to a caveolae-rich fraction within the plasma cell membrane: implications for type II diabetes", Mol. Med. 2(3):367-372 (May 1996)
17. Ganong, William F., MD, Review of Medical Physiology, 19th edition, 1999, p. 9, pp. 26-33
18. Pan, D.A. et al., "Skeletal muscle membrane lipid composition is related to adiposity and insulin action", J. Clin. Invest. 96(6):2802-2808 (December 1995)
19. Physicians' Desk Reference, 53rd edition, 1999
20. Smith, Thomas, Insulin: Our Silent Killer, Thomas Smith, Loveland, Colorado, revised 2nd edition, July 2000, p. 20
21. Law Offices of Charles H. Johnson & Associates (telephone 1 800 535 5727, toll free in North America)
22. American Heart Association, "Diabetes Mellitus Statistics", https://www.amhrt.org
23. Shanmugasundaram, E.R.B. et al. (Dr Ambedkar Institute of Diabetes, Kilpauk Medical College Hospital, Madras, India), "Possible regeneration of the Islets of Langerhans in Streptozotocin-diabetic rats given Gymnema sylvestre leaf extract", J. Ethnopharmacology 30:265-279 (1990); Shanmugasundaram, E.R.B. et al., "Use of Gemnema sylvestre leaf extract in the control of blood glucose in insulin-dependent diabetes mellitus", J. Ethnopharmacology 30:281-294
(1990)
24. Smith, ibid., pp. 97-123
25. Many popular artificial sweeteners on sale in the supermarket are extremely poisonous and dangerous to the diabetic; indeed, many of them are worse than the sugar the diabetic is trying to avoid; see, for example, Smith, ibid., pp. 53-58.
26. Walker, Morton, MD, and Shah, Hitendra, MD, Chelation Therapy
27. Expensive but Delicious ~ A little goes a long way: May this website author also suggest Gourmet Virgin Tea Oil?
28. Your source for research on the health benefits of coconut
oil: https://www.coconutoil.com/
29. Virgin Coconut Oil: The Healthy Oil for Diabetes by Bruce Fife, N.D.
(
), Keats Publishing, Inc., New Canaan, Connecticut, 1997, ISBN 0-87983-730-6
Fats and Oils
Fats and oils are an important part of any well designed dietary plan. A good working understanding of just what they are and how they work is an essential part of any well conceived diet. Fats and oils, certainly as much and perhaps more than any other single dietary component, directly
impact our health in profound ways.
The difference between fats and oils is in their melting point. Fats tend to be solids at room temperature; oils tend to be liquid at room temperature. To turn a fat into an oil, merely raise its temperature above its melting point. If the temperature continues to increase beyond the melting point to the point where some smoke becomes evident, the molecular structure of the oils will change and a number of toxic molecular isomers will be produced in the oil. If the oil is allowed to cool or to resolidify, the toxic products will remain. The temperatures where this damage is done to our fats and oils is about half the temperatures reached in the refining and Hydrogenation processes (part of the aforementioned "" of greed). Thus, these processes routinely destroy all of the nutritional value of our fats and oils. These refined and/or Hydrogenated fats and oils are characterized by an extraordinarily long shelf life; some are virtually un spoilable (e.g. "vegetable" oil, "canola" {a.k.a. oilseed or lear} oil, "safflower" oil, peanut oil, etc...).
Naturally occurring fats and oils are Triglycerides. Triglycerides consist of three fatty acids bound to a Glycerol backbone. Each fatty acid consists of a Carbon-Hydrogen chain with a Carboxyl group at the end that is attached to the Glycerol molecule. The other end is typically terminated with a Hydrogen bond. Unless changed chemically, by artificial technology, this is the natural form which we find in the fats and oils that are nutritionally useful. The length of the fatty acid chain as well as its configuration and relative degree of saturation determine how the fatty acid will act within our body. Some fatty acids are vitally necessary to life processes; some are poisons.
Fatty acids are also found in other molecules besides Triglycerides. For example Phospholipids have two fatty acids and a Phosphorus molecule attached to the Glycerol backbone. Phospholipids too, play an important role in our cellular health.
Understanding Triglycerides is an important issue that is complicated by a great deal of pseudo science that is specifically designed to confuse and mislead. In addition to the Triglycerides that we eat in the form of fats and oils, we also have Triglycerides formed, within our bodies, from the
sugars and starches that we eat. Much of this Triglyceride load is deposited in our adipose (fat) cells when we eat too much fat and sugar and some of us become obese. Some of these Triglycerides are broken down into their fatty acids which are then used in cell repair. When we lack CIS type w=3's in our diet, most of the fatty acid load is either trans-fats or saturated fats; these are used to repair our cell membranes. It is the combined absence of the CIS w=3 fats and oils and the presence of these saturated and trans-fats and other toxic isomers that cause these cellular membranes to become stiff and sticky instead of fluid and slippery. Additional biochemical detail on this cellular membrane issue is
discussed on the above diabetes article.
The saturated fat Triglycerides circulate in the blood stream before finding a home in our Adipose cells (fat cells). They tend to be sticky instead of slippery and so contribute to the high incidence of Strokes and Atherosclerosis associated with high levels of Triglycerides in the blood. They
make the blood viscosity thicker and cause the Platelets to tend to stick together. They are also an essential step in the chain of events that cause obesity.
All dietary fatty acids may be divided into two categories:
Saturated and Unsaturated. The Unsaturated fats and oils differ from each other in their configuration and in their degree of unsaturation. Both types of fatty
acids are produced by the the animal and by the vegetable kingdoms, although some are predominately found in animal sources and some are predominately found in vegetable sources. Most concentrated vegetable sources are seeds and nuts; most animal sources are animal body fat. Unrefined fish oils are good sources of dietary CIS w=3 fats; unrefined Flax seed oil, Hemp seed oil and several others are good concentrated vegetable sources of CIS w=3 oils (which makes our corporate food system a dictatorship since the big chain grocery stores have summarily removed most of these healthy oils from the shelves).
Saturated fats are characterized by having all of the possible molecular locations for a Hydrogen bond filled. Thus, at the molecular level, there is no molecular difference between a saturated vegetable fat or a saturated animal fat of the same chain length. There also is no molecular
difference between a natural and an artificial saturated fat of the same chain length. Configuration is not an issue because when all of the bonds are filled there is only one configuration possible. As the length of the fatty acid chain lengthens the melting point of the fat increases. Thus fats which are solid at room temperature have longer chain lengths than fats which are liquid at room temperatures. Our bodies can readily process short and medium chain fats; but, it processes longer chain fats with greater difficulty.
However, with animal sources, vegetable sources and even with artificially made dietary sources, single individual fat molecules are never found. We must always deal with mixtures of many different fat and oil molecules in the fats and oils that we consume. All naturally occuring fats and oils are mixtures of long and short chain saturated fats and mixtures of mono and poly unsaturated fats of the CIS configuration. Naturally occuring trans-isomers are relatively rare and do not occur in sufficient abundance to create a health hazard. However if fats and oils are refined, heated or Hydrogenated, the mixtures are then made to also include a huge thermodynamic distribution of highly toxic isomers, including the notorious trans-isomer, along with partially destroyed molecular fragments, and other toxic products. (Food products are beginning to be labelled "No Trans Fat!" but we still need to question the possible presence of other toxic substances: Examine the ingredients and ask the manufacturer about suspected oils.)
All fats and oils differ from each other in the length of the Carbon-Hydrogen chain; however, unsaturated fats and oils also differ from each other, and from saturated fats, in that they have one or more vacant Hydrogen sites along their chain. These unfilled Hydrogen binding sites give the
unsaturated fats and oils a variety of geometries at the molecular level. Some of these geometries, notably the "CIS" geometries that occur naturally in nature and are designed so that our metabolism can readily handle them, in fact, it needs them. Certain CIS type unsaturated oils, the w=3's, directly constitute an important building block in all of the sixty seven or so trillion cells in our body, and they cannot be obtained by our body except from our food supply. In addition, our enzyme systems use unsaturated fats as building blocks to construct a wide variety of needed biochemicals.
Short and medium chain length saturated animal fats are a very nutritious food staple and have been for thousands of years. They provide nine calories per gram and are "good keepers"; in the days before refrigeration, this "keeping" quality was very important. It meant that the fat would not spoil or go rancid easily at room temperature. Our body uses saturated fats as a highly concentrated energy source when carbohydrates not plentiful. Much of the disease we experience today is the result of a failure of our systems to properly and safely metabolize fats and oils (e.g. diabetes). Rather than use them for the highly concentrated energy source that they are, our body uses them in cell repair
because the CIS w=3's are not in our diet. This is now identified as a major factor in Hyperinsulinemia.
Cholesterol is a fatty substance that is manufactured by our liver. It is an extremely important building block for many of our vital functions including our brains, eyes, nervous systems and sexual apparatus (both varieties). About 85% of the Cholesterol circulating in our bodies is made by the liver. We have a Cholesterol control mechanism in our bodies that operates to stabilize Cholesterol at the circulating level that we find. Cholesterol is also contained in some of the foods that we eat. If we try to reduce our circulating Cholesterol by excluding high Cholesterol foods from our diet, our liver simply makes more Cholesterol in an attempt to maintain a homeostasis (normal level) of Cholesterol in our blood stream. Controlling circulating Cholesterol through diet is like trying to empty the ocean with a teaspoon; it sounds like a good pop science theory but it is really not very effective.
Here are important questions we need to ask about cholesterol before we jump on another health trend band wagon:
Now, it's very important to ask yourself when you read trendy, pop science articles such as the following, "Who is really gaining from the proliferation of this 'bad' cholesterol propaganda?"
{While you are reading the following article please notice that the author never attempts to define or even spell out low density lipoprotein, never attempts to explain the purpose of LDLs in the body, never attempts to explain how LDLs are manufactured or regulated in the body, AND never attempts to explain the diet and lifestyle that can throw cholesterol levels off kilter. In essence, this is propaganda because it does not attempt to educate the public, but constantly refers to LDLs as a bad fat although it is manufactured by the liver in every healthy body and this article influences the public to take more statins to make the pharmaceutical companies richer. This Propaganda is most dangerous since it takes a position within respected media such as the NY Times with "experts" backing up the claim to "do the right thing."}
As we shall see elsewhere in this website and in our special report Insulin: Our Silent Killer the best way to reduce Cholesterol levels to normal is to cure the underlying Hyperinsulinemia. This entails repairing the Automatic Cholesterol Control System which regulates our Cholesterol homeostasis. This repair process requires stabilizing our blood Insulin and Glucose levels and restoring our entire endocrine system to proper
balance. This follows automatically when we stop consuming dangerous, damaged fats and oils and restore other needed nutrition to our diet.
Cholesterol, being a fat, does not dissolve in the blood stream which is mostly water. In order to be transported around in the blood, it must be carried by a Lipoprotein carrier which has an affinity for water. When it is being carried from the liver to the rest of the body, the Lipoprotein involved is LDL (low density Lipoprotein). When Cholesterol is being carried from the body back to the liver for recycling, the carrier is HDL (high density Lipoprotein). Thus LDL which distributes Cholesterol throughout the body came to be known as the "bad" Cholesterol and HDL which removes it from circulation came to be known as the "good" Cholesterol. Hyperinsulinemia is characterized by a reduction in the HDL fraction and an increase in the LDL fraction. Clearly this sort of phony science that characterizes one essential Lipoprotein as "good" and another as "bad" is the sort that comes from marketing and sales departments; certainly it does not originate in reputable scientific laboratories.
Besides being a most important building block in many of our bodily functions, Cholesterol is one of the important components of the plaque that occludes our arteries. It is for this reason that it has attracted notice. Our diseased state is due to the fact that the normal levels of circulating Cholesterol have been elevated by Hyperinsulinemia. In fact, this elevated level of Cholesterol is often one of the early warning signs that we are becoming Hyperinsulinemic. An appropriate way to reduce Cholesterol is to cure the underlying Hyperinsulinemia.
With the advent of artificial fats and oils and Hydrogenated and Refined products in the 1920's (see history), the CIS type w=3 unsaturated oils started to disappear from our dietary food chain and were replaced by a large number of toxic isomers. These toxic isomers are just different geometries of the unsaturated oil molecules many of which were, before
processing, of the CIS type. Long term consumption of some of these toxic isomers, notably the trans-isomer, has been identified with many, if not most, of the chronic disease symptoms discussed on this home page. Of even greater importance, the complete removal of some of the CIS type w=3 oils from our diet has been found to be causal in many of our widespread degenerative diseases including Hyperinsulinemia.
Some of the biochemical effects of these toxic isomers are discussed on the diabetes page.
Much of this came about because of standardized refining processes that were introduced into the oils manufacturing business. The new rapid high temperature extraction techniques, introduced in the 1920's lowered the retail price of oil, gave it a pure pristine appearance when packaged in a transparent bottle, gave it a uniform clarity, gave it an almost uniform taste, and destroyed the CIS w=3 fatty acids that rapidly spoiled at room temperature. It is the high temperatures used in the refining process that ruins even previously good oils. If we find a good oil and refrigerate it, it is still easy to destroy its nutritional qualities when we cook with it by heating it to the point where it smokes. When delicate CIS w=3 oils are over heated, either in cooking or refining, the oil undergoes irreversible changes; the CIS configuration is destroyed and many toxic isomers are generated, including the notorious trans-isomer. All of the antioxidents, previously a part of the unrefined oil are destroyed. Much of the oil's original flavor is lost and it tastes like a generic oil.
When cooking with fats and oils it is important to do so in a manner that does not destroy them. Use only butter, Coconut oil and animal fat for cooking. These contain a higher proportion of saturated fat and thus are not destroyed as easily at cooking temperatures. Never consume any deep fried foods; they are all universally soaked with toxic isomers (Use that deep fryer for boiling and steaming). If you cook with an oil like olive oil, be sure to mix some water with it to prevent the oil from getting too hot. Remember that if the oil starts to smoke it is too hot and it is being
destroyed.
To cure Hyperinsulinemia, Type II Diabetes, Syndrome X and many other consequential diseases that stem from poisonous fats and oils, it is important to realize that the chronic ingestion of Refined and Hydrogenated fats and oils is implicated as a causal agent in these diseases. Margarine, artificial shortenings, refined oils and all Hydrogenated edible products are long term toxic to the human metabolism (the longer the shelf life, the shorter the human life). Any unsaturated fat or oil that does not need constant refrigeration should be considered inedible. Many saturated fats and oils, while also benefiting from refrigeration, do not turn rancid nearly so easily as CIS w=3 type unsaturated fats and oils at room temperature.
An important consideration about these edible oils is a widespread fraudulent advertising technique that enables the oils manufacturer to sell known toxic oils to the unsuspecting public without breaking the law (in the same way fluoride is marketed by "approval" of certain government "health" agencies). Many refined vegetable oils are advertised as mono unsaturated or as polyunsaturated in order to confuse the purchaser. Indeed, if these oils were the CIS isomer, they would be desirable oils from a health standpoint. However, CIS type w=3 oils are inherently unstable and will go rancid quite rapidly in a transparent bottle on a room temperature grocery store shelf; their shelf life is on the order of ten hours or sometimes less (like milk or eggs). The trans-isomer of these oils has a much longer room temperature shelf life. There is no law to require the oils manufacturer, or the store, to advise the consumer that these "monounsaturates" and "polyunsaturates" are trans-isomers and other toxic byproducts that result from the destruction of the good edible oils that they think they are getting. Since no law exists to keep their claims honest, oils manufacturers feel free to deceive with dishonest claims that few consumers understand. In some circles this is not considered to be fraud. {Update: According to an official response from the American Diabetes Association standardized labeling of food products containing toxic isomers begins in 2006.}
In our discussion on Hyperinsulinemia we discuss more about the fat and oil issue and cover in detail ways we can protect ourselves from the consequences of the fraudulent advertising claims with which we are constantly bombarded. We also discuss how to reverse the degenerative process in the event we are involved with it.
More information is available in our hardcopy Special Report for those who have a compelling interest or who simply wish to know more about the health connection to our dietary fats and oils.
References:
Erasmus U PhD, "Fats that heal Fats that kill" (
), Alive Books, 7436 Frazer
Park Drive, Burnaby BC, Canada 1996
Johnston JR PhD, Johnson IM CN, "Flaxseed (Linseed) oil and the power of omega-3," (
) Keats publishing, Inc. New Canaan, Connecticut.
Beck JS, "Biomembranes: Fundamentals in relation to human biology." NY, NY
McGraw-Hill 1980
Enig MG, "Trans fatty acids in the food supply: A comprehensive report covering 60 years of research.", Enig Associates, Inc. Silver Springs, MD 1993
Okolska G et al, "[Current recommendations concerning the rational use of fats. II. Value of polyunsaturated fatty acids from the n=6 and n=3 groups and general recommendations]. Rocz Panstw Zakl Hig 1989;40(3):178-187
 Naturally occurring fats and oils are Triglycerides. Triglycerides consist of three fatty acids bound to a Glycerol backbone. Each fatty acid consists of a Carbon-Hydrogen chain with a Carboxyl group at the end that is attached to the Glycerol molecule. The other end is typically terminated with a Hydrogen bond. Unless changed chemically, by artificial technology, this is the natural form which we find in the fats and oils that are nutritionally useful. The length of the fatty acid chain as well as its configuration and relative degree of saturation determine how the fatty acid will act within our body. Some fatty acids are vitally necessary to life processes; some are poisons.
Naturally occurring fats and oils are Triglycerides. Triglycerides consist of three fatty acids bound to a Glycerol backbone. Each fatty acid consists of a Carbon-Hydrogen chain with a Carboxyl group at the end that is attached to the Glycerol molecule. The other end is typically terminated with a Hydrogen bond. Unless changed chemically, by artificial technology, this is the natural form which we find in the fats and oils that are nutritionally useful. The length of the fatty acid chain as well as its configuration and relative degree of saturation determine how the fatty acid will act within our body. Some fatty acids are vitally necessary to life processes; some are poisons. Fatty acids are also found in other molecules besides Triglycerides. For example Phospholipids have two fatty acids and a Phosphorus molecule attached to the Glycerol backbone. Phospholipids too, play an important role in our cellular health.
Fatty acids are also found in other molecules besides Triglycerides. For example Phospholipids have two fatty acids and a Phosphorus molecule attached to the Glycerol backbone. Phospholipids too, play an important role in our cellular health. Cholesterol is a fatty substance that is manufactured by our liver. It is an extremely important building block for many of our vital functions including our brains, eyes, nervous systems and sexual apparatus (both varieties). About 85% of the Cholesterol circulating in our bodies is made by the liver. We have a Cholesterol control mechanism in our bodies that operates to stabilize Cholesterol at the circulating level that we find. Cholesterol is also contained in some of the foods that we eat. If we try to reduce our circulating Cholesterol by excluding high Cholesterol foods from our diet, our liver simply makes more Cholesterol in an attempt to maintain a homeostasis (normal level) of Cholesterol in our blood stream. Controlling circulating Cholesterol through diet is like trying to empty the ocean with a teaspoon; it sounds like a good pop science theory but it is really not very effective.
Cholesterol is a fatty substance that is manufactured by our liver. It is an extremely important building block for many of our vital functions including our brains, eyes, nervous systems and sexual apparatus (both varieties). About 85% of the Cholesterol circulating in our bodies is made by the liver. We have a Cholesterol control mechanism in our bodies that operates to stabilize Cholesterol at the circulating level that we find. Cholesterol is also contained in some of the foods that we eat. If we try to reduce our circulating Cholesterol by excluding high Cholesterol foods from our diet, our liver simply makes more Cholesterol in an attempt to maintain a homeostasis (normal level) of Cholesterol in our blood stream. Controlling circulating Cholesterol through diet is like trying to empty the ocean with a teaspoon; it sounds like a good pop science theory but it is really not very effective.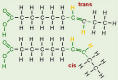 Much of this came about because of standardized refining processes that were introduced into the oils manufacturing business. The new rapid high temperature extraction techniques, introduced in the 1920's lowered the retail price of oil, gave it a pure pristine appearance when packaged in a transparent bottle, gave it a uniform clarity, gave it an almost uniform taste, and destroyed the CIS w=3 fatty acids that rapidly spoiled at room temperature. It is the high temperatures used in the refining process that ruins even previously good oils. If we find a good oil and refrigerate it, it is still easy to destroy its nutritional qualities when we cook with it by heating it to the point where it smokes. When delicate CIS w=3 oils are over heated, either in cooking or refining, the oil undergoes irreversible changes; the CIS configuration is destroyed and many toxic isomers are generated, including the notorious trans-isomer. All of the antioxidents, previously a part of the unrefined oil are destroyed. Much of the oil's original flavor is lost and it tastes like a generic oil.
Much of this came about because of standardized refining processes that were introduced into the oils manufacturing business. The new rapid high temperature extraction techniques, introduced in the 1920's lowered the retail price of oil, gave it a pure pristine appearance when packaged in a transparent bottle, gave it a uniform clarity, gave it an almost uniform taste, and destroyed the CIS w=3 fatty acids that rapidly spoiled at room temperature. It is the high temperatures used in the refining process that ruins even previously good oils. If we find a good oil and refrigerate it, it is still easy to destroy its nutritional qualities when we cook with it by heating it to the point where it smokes. When delicate CIS w=3 oils are over heated, either in cooking or refining, the oil undergoes irreversible changes; the CIS configuration is destroyed and many toxic isomers are generated, including the notorious trans-isomer. All of the antioxidents, previously a part of the unrefined oil are destroyed. Much of the oil's original flavor is lost and it tastes like a generic oil. 
